Learn how to safely manage bleeding risk in cirrhosis during procedures. Explore tips on transfusions, INR correction, and procedure-specific strategies
Peri-Procedural Management of Bleeding Risk in Cirrhosis
Introduction
Patients with cirrhosis are at an increased risk of bleeding during invasive procedures. However, the relationship between liver dysfunction and bleeding risk is complex. Despite abnormalities in conventional coagulation tests (like prolonged INR or low platelet counts), many cirrhotic patients may not bleed excessively — and some may even be prone to clotting.
Effective peri-procedural management requires a careful, individualized assessment to balance bleeding and thrombotic risks, avoid unnecessary delays, and improve outcomes.
________________________________________
Why Is Bleeding Risk Elevated in Cirrhosis?
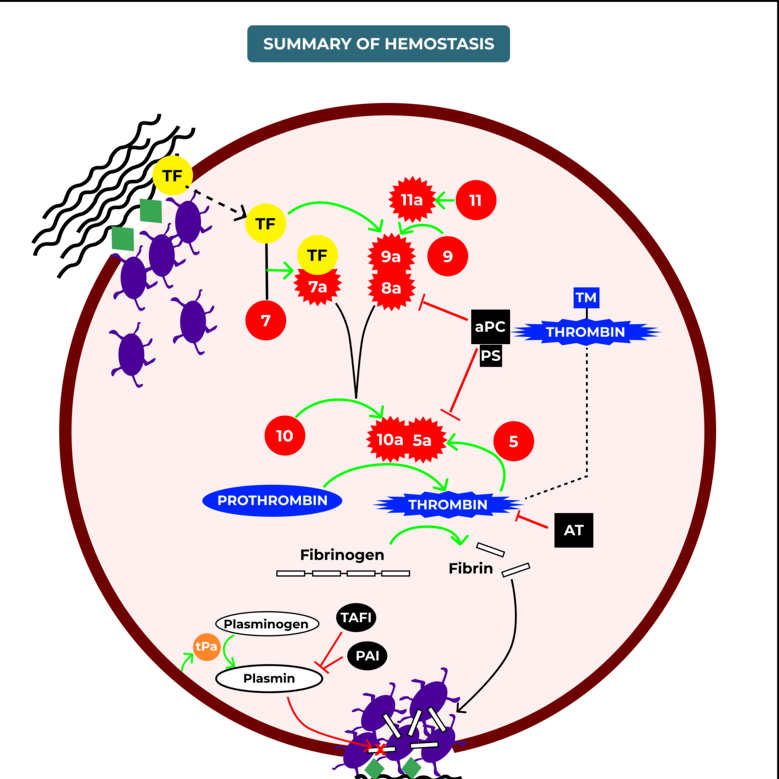
Several changes in cirrhosis contribute to a fragile balance:
• Reduced clotting factors production (e.g., fibrinogen, prothrombin)
• Thrombocytopenia due to splenic sequestration (hypersplenism)
• Reduced platelet function
• Elevated fibrinolysis
• Endothelial dysfunction
At the same time, pro-coagulant factors like Factor VIII and von Willebrand factor are often elevated, meaning the bleeding risk is not purely based on INR or platelet counts alone.
Keywords: coagulopathy in cirrhosis, bleeding and clotting in liver disease
________________________________________
Key Considerations Before a Procedure
1. Assess the Patient’s True Bleeding Risk
• Child-Pugh score and MELD score can give an idea of overall liver dysfunction.
• Thrombocytopenia (platelets <50, 000/µL) increases bleeding risk for high-risk procedures.
• INR alone is not reliable for bleeding prediction in cirrhosis.
• Consider the type of procedure (low-risk vs. high-risk).
2. Risk Stratification by Procedure Type
Low Bleeding Risk High Bleeding Risk
Paracentesis Liver biopsy (transjugular is safer)
Diagnostic endoscopy ERCP with sphincterotomy
Central line placement Variceal band ligation
Thoracentesis Percutaneous tumor ablation
Dental extraction (simple) Neurosurgical procedures
Keywords: procedures safe in cirrhosis, high-risk liver procedures
________________________________________
Management Strategies
1. Platelet Transfusion
• Threshold: Consider if platelets <50, 000/µL before major procedures.
• Some centers use thrombopoietin receptor agonists (e.g., lusutrombopag, avatrombopag) to avoid transfusions.
2. Fresh Frozen Plasma (FFP)
• Limited role — FFP may temporarily correct INR but has minimal impact on bleeding outcomes.
• Can worsen fluid overload and portal hypertension.
• Generally reserved for massive bleeding, not prophylactic use.
3. Cryoprecipitate
• Consider if fibrinogen <100 mg/dL before major surgery or biopsy.
4. Vitamin K
• Only useful if Vitamin K deficiency is suspected (e.g., cholestasis, poor nutrition).
5. Tranexamic Acid
• Antifibrinolytic agents may help in selected cases (ongoing bleeding), but prophylactic use remains controversial.
________________________________________
Practical Approach Before Common Procedures
✅ Paracentesis/Thoracentesis:
• Safe even with low platelets and elevated INR. Routine correction not needed unless platelets <20, 000/µL.
✅ Endoscopy (no intervention):
• Generally safe. No need for correction unless active variceal bleeding anticipated.
✅ Endoscopic Therapy (Banding, ERCP):
• Aim for platelets >50, 000/µL if possible. INR correction usually unnecessary.
✅ Liver Biopsy:
• Prefer transjugular approach in high-risk patients.
• If percutaneous, aim for platelets >50, 000/µL and fibrinogen >100 mg/dL.
________________________________________
Emerging Tools
• Viscoelastic tests like TEG (Thromboelastography) and ROTEM offer better insight into real-time coagulation status than INR/PT.
• Still not widely available, but gaining popularity for peri-procedural decisions.
Keywords: TEG in liver disease, thromboelastography bleeding risk
________________________________________
Conclusion
Managing bleeding risk in patients with cirrhosis undergoing procedures requires individualized, evidence-based strategies. Routine correction of abnormal INR or low platelets is often unnecessary for low-risk procedures.
Careful planning, appropriate transfusion thresholds, and choosing safer procedural techniques (like transjugular approaches) can greatly reduce complications.
Emerging tests like TEG/ROTEM may further personalize care in the near future.
By balancing caution with pragmatism, healthcare providers can ensure that necessary procedures are performed safely — without undue fear of bleeding.
________________________________________
Frequently Asked Questions (FAQs)
Q1. Is paracentesis safe in cirrhosis patients with high INR?
Yes. Large-volume paracentesis is considered safe even with elevated INR and thrombocytopenia.
Q2. Should INR always be corrected before procedures in liver disease?
No. INR does not reliably predict bleeding risk in cirrhosis. Correction should be based on procedure type and clinical judgment.
Q3. When should platelet transfusions be given before procedures?
For major interventions, transfusions are considered if platelet count is below 50, 000/µL.
Q4. What is the safest way to biopsy the liver in cirrhosis patients?
The transjugular liver biopsy is preferred in high-risk cases to minimize bleeding risk.
________________________________________